
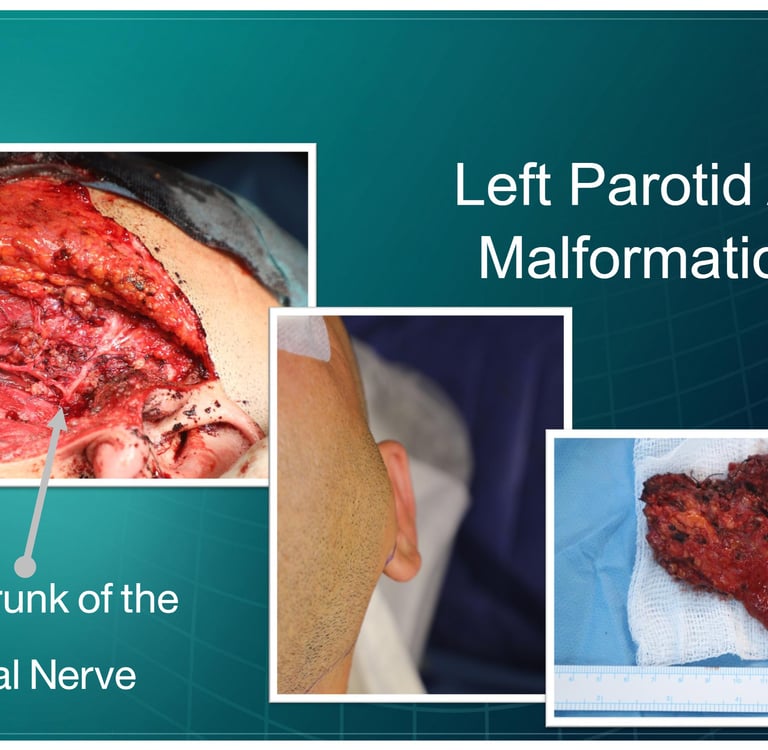
Left Parotid AV Malformation in a 32-Year-Old Male
A 32-year-old male presented with a left preauricular swelling that has been progressively changing in size over the past four years, accompanied by pulsatile tinnitus. He reported no known drug allergies and denied any recent flu-like symptoms. The chronicity of the swelling and associated symptoms suggested a vascular malformation, likely an arteriovenous malformation.
SURGERYHEAD AND NECKVIDEO
7/15/20262 min read

Patient Presentation:
A 32-year-old male presented with a left preauricular swelling that has been progressively changing in size over the past four years, accompanied by pulsatile tinnitus. He reported no known drug allergies and denied any recent flu-like symptoms. The chronicity of the swelling and associated symptoms suggested a vascular malformation, likely an arteriovenous malformation.
Laboratory Investigations:
Lab results indicate a compatible cross-matching test. Hematology results show WBC at 6.0 10^9/L, with normal lymphocyte and granulocyte percentages. Thyroid function tests reveal TSH at 2.55 uIU/ml, within normal limits. Renal function tests show blood urea at 28.4 mg/dl, which is also in normal range. Serum glucose is at 77.8 mg/dl, normal for fasting levels. Viral screening shows non-reactive results for HIV, HCV, and HBs antigens.
Ultrasound Findings:
Ultrasound of the neck revealed an ill-defined hypoechoic hypervascular nodule measuring approximately 38 × 20 × 23 mm in the posterior medial aspect of the left parotid gland, associated with dilated tortuous vessels suggestive of vascular malformation or hemangioma. No significant cervical lymphadenopathy was noted. The thyroid gland and other salivary glands appeared normal.
MRI Findings of the Neck:
Imaging findings demonstrate a left preauricular arteriovenous malformation (AVM), characterized by dilated and tortuous vascular channels supplied by branches of the left external carotid artery, with associated enlargement of the left parotid gland vasculature. Additionally, there is marked inflammatory involvement of the left external auditory canal with complete luminal obliteration, accompanied by diffuse opacification of the left mastoid air cells, consistent with associated otomastoid inflammatory changes. No mass lesion is identified within the nasopharynx, oropharynx, or hypopharynx. The oral cavity, tongue base, right parotid gland, bilateral submandibular glands, and visualized brain parenchyma are unremarkable.
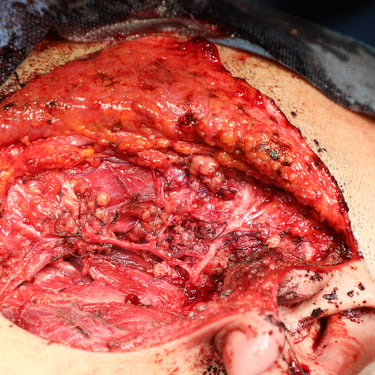
Surgical Management:
The patient underwent Left parotidectomy under general anesthesia through a lazy S incision. Intraoperatively, the facial nerve and its major branches were meticulously identified and preserved. Adequate hemostasis was achieved, and a corrugated drain was placed in the operative bed. The wound was closed in anatomical layers. The patient tolerated the procedure well, with no reported intraoperative complications, and intraoperative findings were consistent with the preoperative imaging.
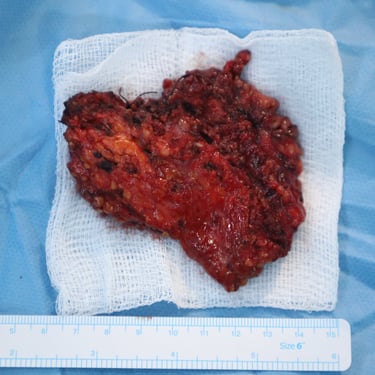
Histopathological Examination:
Histopathology of the parotid tissue revealed benign salivary gland tissue with reactive lymph nodes and vascular malformation in the soft tissue. No malignancy was identified, confirming the diagnosis of a benign vascular malformation.
Postoperative Course and Follow-Up:
The patient had a stable postoperative recovery without significant complications. Vital signs remained stable, and he was discharged with follow-up recommendations for monitoring the surgical site and any potential recurrence of symptoms. He was advised to maintain regular check-ups to assess for any further vascular issues.



Address
Majid Bag Main Street, Beside University of Sulaymaniyah Old Campus, Madam Mitterrand, Sulaymaniyah, Iraq
Contacts
info@ssthyroid.com

